

Background:
Allogeneic hematopoietic cell transplant (HCT) is a potentially curative approach for eligible patients with acute myeloid leukemia (AML). The 5-year overall survival (OS) for AML patients (pts) following HCT is approximately 40-50%. However, data regarding outcomes for pts with certain molecular subtypes of AML are lacking. Of particular interest are post-HCT outcomes of pts with targetable mutations such as FLT3, IDH1, or IDH2, given the potential role of maintenance targeted therapy in the post-HCT setting. We conducted a retrospective, multi-institutional study describing outcomes for IDH1- or IDH2-mutated AML pts following HCT.
Methods:
We performed retrospective data collection, using institutional databases, at three academic sites (Massachusetts General Hospital, Dana Farber Cancer Institute, and Ohio State University). We identified pts >18 years of age with a diagnosis of IDH1- or IDH2-mutated AML who underwent allogeneic HCT from 2010 to 2019. Data collected included pt age, sex, mutational and cytogenetic profile, treatment received prior to HCT, marrow response prior to HCT, stem cell source, HCT conditioning regimen, graft-versus-host disease (GVHD) prophylaxis, and time of relapse, death, or last known follow-up. IDH mutational status was assessed using next generation sequencing prior to HCT. Time to event endpoints are analyzed using the Kaplan Meier method for OS and progression-free survival (PFS), or the Gray method in a competing risk setting for time to relapse and non-relapse mortality (NRM). Proportional hazard cox models and competing risk regression models were used to test difference between groups while adjusting for other covariates.
Results:
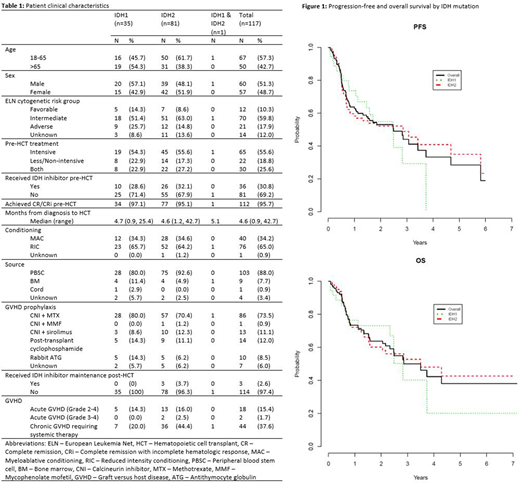
In total, 117 pts with IDH1- or IDH2-mutated AML who received allogeneic HCT were identified. An IDH1 mutation was identified in 35 patients (pts) while an IDH2 mutation was found in 81 pts (Table 1). One pt had both IDH1 and IDH2 mutations and he was not included in subsequent univariate and multivariate analyses. The most commonly co-occurring mutations among all patients were DNMT3A (35%), NPM1 (32%), FLT3-ITD (14%), ASXL1 (10%), and TP53 (3%). 50 pts (43%) were >65 years old (range 27-74), and 60 (51%) were male. 12 pts (10%) had favorable-risk, 70 pts (60%) had intermediate-risk, and 21 pts (18%) had adverse-risk AML by ELN cytogenetic criteria; data were unavailable for 14 patients (12%). 112 pts (96%) achieved CR/CRi prior to HCT. 76 pts (65%) received reduced intensity and 40 (34%) underwent myeloablative conditioning (Table 1); data were unavailable for 1 patient (0.9%). 36 pts (31%) received an IDH inhibitor before HCT and 3 (2.6%) received an IDH inhibitor as maintenance therapy after HCT. Following HCT, 18 pts (15%) experienced grade 2-4 acute GVHD and 44 (38%) experienced chronic GVHD requiring systemic treatment. With a median follow-up of 23 months for surviving pts, the 1-year PFS and OS for the IDH1-mutated cohort was 74% (95% CI 55%-85%) and 76% (95% CI 58%-87%), respectively, and the 2-year PFS and OS was 55% (95% CI 35%-71%) and 73% (95% CI 55%-85%), respectively (Figure 1). With a median follow-up of 26 months for surviving pts, the 1-year PFS and OS for the IDH2-mutated cohort was 58% (95% CI 47%-68%) and 72% (95% CI 61%-81%), respectively, and the 2-year PFS and OS was 52% (95% CI 40%-63%) and 60% (95% CI 48%-70%), respectively (Figure 1). The 2-year cumulative incidence of relapse and NRM was 36.1% (95% CI 19.0%-53.6%) and 9.1% (95% CI 2.2%-22.0%), respectively, for the IDH1-mutated cohort, and 29.8% (95% CI 19.9%-40.4%) and 18.0% (95% CI 10.3%-27.3%), respectively, for the IDH2-mutated cohort. On multivariate analysis of OS, there was no statistically significant association with older age, higher-risk disease, absence of pre-HCT CR/CRi, use of reduced intensity conditioning, or IDH mutation.
Conclusion:
This is the first multi-institutional retrospective study to characterize outcomes of IDH1- or IDH2-mutated AML patients undergoing allogeneic HCT. We report important benchmarks of relapse, disease-free, and overall survival that will inform interpretation of ongoing and future clinical trials investigating the benefit of maintenance IDH1 and IDH2 inhibitor therapy in the post-HCT setting.
Eisfeld:Karyopharm: Current Employment, Current equity holder in publicly-traded company; Vigeo Therapeutics: Consultancy. Mims:Novartis: Speakers Bureau; Agios: Consultancy; Leukemia and Lymphoma Society: Other: Senior Medical Director for Beat AML Study; Abbvie: Membership on an entity's Board of Directors or advisory committees; Kura Oncology: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Other: Data Safety Monitoring Board; Syndax Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees. Jones:Pharmacyclics LLC, an AbbVie Company: Patents & Royalties: and other intellectual property, Research Funding. Cutler:Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees; Kadmon: Consultancy, Membership on an entity's Board of Directors or advisory committees; Jazz: Consultancy, Membership on an entity's Board of Directors or advisory committees; Medsenic: Consultancy, Membership on an entity's Board of Directors or advisory committees; Generon: Consultancy, Membership on an entity's Board of Directors or advisory committees; Mesoblast: Consultancy, Membership on an entity's Board of Directors or advisory committees. Koreth:Amgen: Consultancy; Moderna Therapeutics: Consultancy; Biolojic Design Inc: Consultancy; EMD Serono: Consultancy; Equillium: Consultancy; Clinigen: Other; Miltenyi: Other: Research Support; BMS: Other: Research Support; Cugene: Membership on an entity's Board of Directors or advisory committees; Therakos: Membership on an entity's Board of Directors or advisory committees; Regeneron: Other: Research Support. Defilipp:Incyte: Research Funding; Regimmune: Research Funding; Syndax Pharmaceuticals: Consultancy. Soiffer:Celgene: Membership on an entity's Board of Directors or advisory committees; Rheos Therapeutics: Consultancy; Juno: Membership on an entity's Board of Directors or advisory committees; alexion: Consultancy; Be the Match/ National Marrow Donor Program: Membership on an entity's Board of Directors or advisory committees; Gilead: Consultancy; Cugene: Consultancy; Precision Bioscience: Consultancy; Kiadis: Membership on an entity's Board of Directors or advisory committees; VOR Biopharma: Consultancy; Mana Therapeutics: Consultancy; Novartis: Consultancy. Chen:AbbVie: Other: Data and Safety Monitoring Board Member; Equillium: Other: Data and Safety Monitoring Board Member; Takeda: Consultancy; Incyte Corporation: Consultancy; Magenta: Consultancy; Kiadis: Consultancy; Actinium: Other: Data and Safety Monitoring Board Member. Fathi:PTC Therapeutics: Consultancy; Daiichi Sankyo: Consultancy; Abbvie: Consultancy; Takeda: Consultancy, Research Funding; Trillium: Consultancy; Forty Seven: Consultancy; Novartis: Consultancy; Amphivena: Consultancy; Astellas: Consultancy; BMS/Celgene: Consultancy, Research Funding; Kite: Consultancy; Trovagene: Consultancy; Boston Biomedical: Consultancy; Kura Oncology: Consultancy; Blueprint: Consultancy; Jazz: Consultancy; Pfizer: Consultancy; Newlink Genetics: Consultancy; Agios: Consultancy, Research Funding; Seattle Genetics: Consultancy, Research Funding; Amgen: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal